
7 results
Gender differences in psychosocial determinants of hand hygiene among physicians
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 45 / Issue 2 / February 2024
- Published online by Cambridge University Press:
- 04 October 2023, pp. 215-220
- Print publication:
- February 2024
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
The effectiveness of the appropriate prophylactic antibiotic use program for surgery
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 3 / Issue S2 / June 2023
- Published online by Cambridge University Press:
- 29 September 2023, pp. s17-s18
-
- Article
-
- You have access
- Open access
- Export citation
-
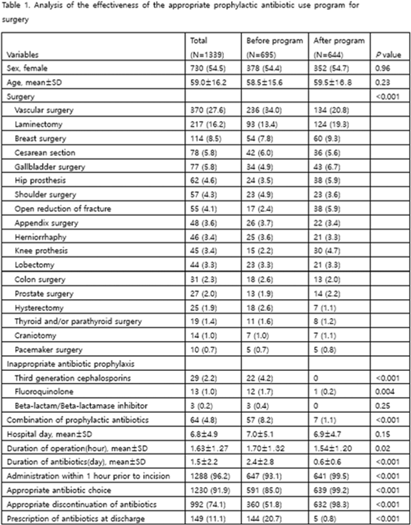
Background: Evaluation of the adequacy of prophylactic antibiotics in surgery has been implemented as a national policy in Korea since August 2007, and the appropriate use of prophylactic antibiotics has improved. However, antibiotic prescriptions that are not recommended or discontinuation of prophylactic antibiotic administration within 24 hours after surgery are still not well done. This study introduced a program to improve the adequacy of prophylactic antibiotics for surgery and analyzed its effects. Methods: We retrospectively analyzed the effectiveness of the appropriate prophylactic antibiotic use program for surgery conducted at a university hospital in Seoul. The participants were patients aged ≥18 years who underwent any of 18 types of surgery. The program started was implemented in June 2020. First, a computer system was used to confirm the antibiotic prescription recommended for each surgery. It also assessed whether the number of days of administration was exceeded, whether antibiotics were prescribed in combination, and whether antibiotics prescribed for discharge medicine were checked in 4 steps. A pop-up window appeared in each patient record to enter the reason for the prescription. If the reason was appropriate, the prescription was allowed, but if not, the prescription was restricted. In addition, infectious diseases physicians and an insurance review team visited each department to conduct an education session. To analyze the effect 3 months before activity (January–March 2020) and 3 months after activity (October–December 2020), we compared the first antibiotic administration rate within 1 hour prior to skin incision, the recommended prophylactic antibiotic administration rate, and surgery type. The rate of discontinuation of prophylactic antibiotics within 24 hours after administration and the rate of prescription of prophylactic antibiotics at discharge were compared. Results: In total, 1,339 surgeries during the study period were included in the analysis. There were 695 cases before the introduction of the program and 644 cases after the introduction. The rate of first antibiotic use within 1 hour prior to skin incision was 93.1%–99.5% (P < .001), the rate of recommended prophylactic antibiotic administration was 85.0%–99.2% (P < .001), and the rate of discontinuation of antibiotic administration within 24 hours after surgery improved from 51.8% to 98.3% (P < .001), respectively. The prescription rate of antibiotics at discharge improved from 20.7% to 0.8% (P <.001) (Table 1). Conclusions: A computerized program to improve the adequacy of prophylactic antibiotic use in surgery combined with education of medical staff was very effective.
Disclosure: None

A SARS-CoV-2 outbreak due to vaccine breakthrough in an acute-care hospital
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 2 / Issue S1 / July 2022
- Published online by Cambridge University Press:
- 16 May 2022, p. s83
-
- Article
-
- You have access
- Open access
- Export citation
-
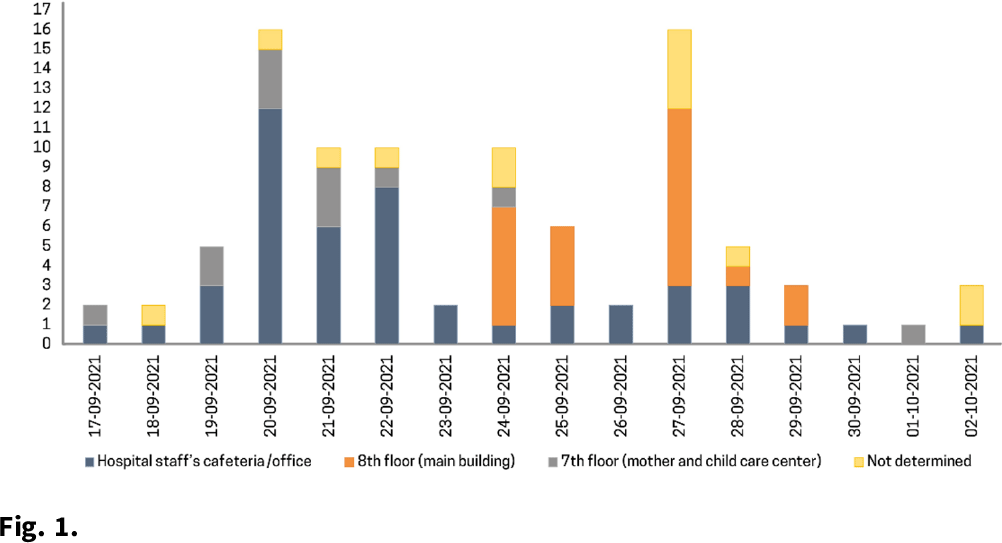
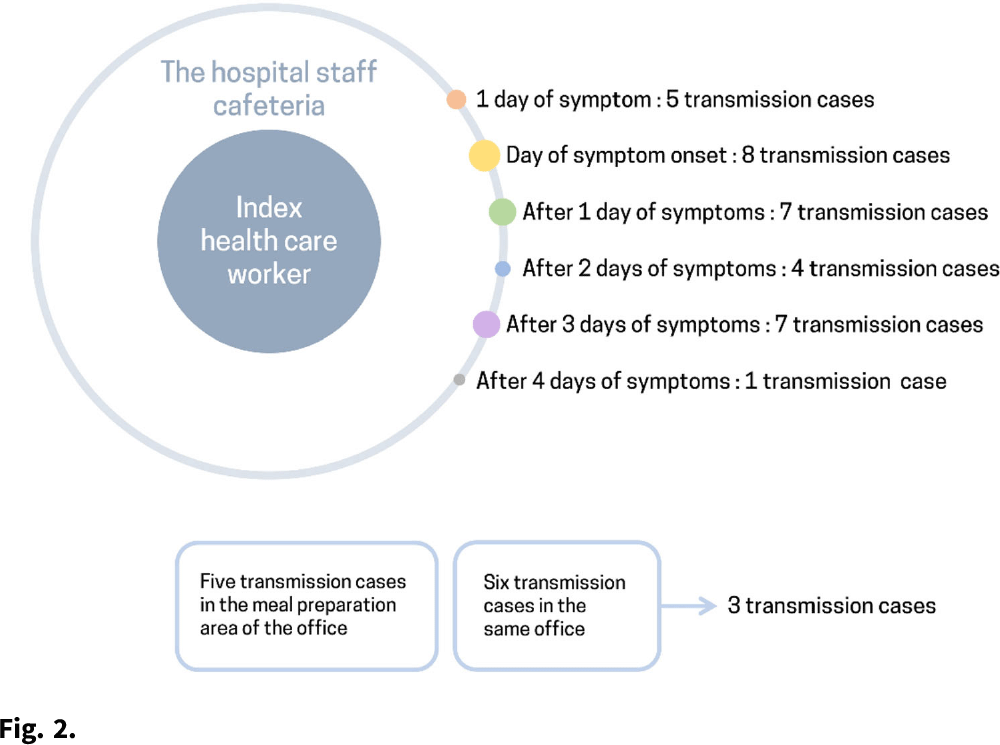
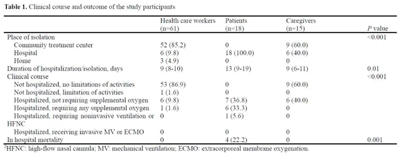
Background: The δ (delta) variant has spread rapidly worldwide and has become the predominant strain of SARS-CoV-2. We analyzed an outbreak caused by a vaccine breakthrough infection in a hospital with an active infection control program where 91.9% of healthcare workers were vaccinated. Methods: We investigated a SARS-CoV-2 outbreak between September 9 and October 2, 2021, in a referral teaching hospital in Korea. We retrospectively collected data on demographics, vaccination history, transmission, and clinical features of confirmed COVID-19 in patients, healthcare workers, and caregivers. Results: During the outbreak, 94 individuals tested positive for SARS-CoV-2 using reverse transcription-polymerase chain reaction (rtPCR) testing. Testing identified infections in 61 health care workers, 18 patients, and 15 caregivers, and 70 (74.5%) of 94 cases were vaccine breakthrough infections. We detected 3 superspreading events: in the hospital staff cafeteria and offices (n = 47 cases, 50%), the 8th floor of the main building (n = 22 cases, 23.4%), and the 7th floor in the maternal and child healthcare center (n = 12 cases, 12.8%). These superspreading events accounted for 81 (86.2%) of 94 transmissions (Fig. 1, 2). The median interval between completion of vaccination and COVID-19 infection was 117 days (range, 18–187). There was no significant difference in the mean Ct value of the RdRp/ORF1ab gene between fully vaccinated individuals (mean 20.87, SD±6.28) and unvaccinated individuals (mean 19.94, SD±5.37, P = .52) at the time of diagnosis. Among healthcare workers and caregivers, only 1 required oxygen supplementation. In contrast, among 18 patients, there were 4 fatal cases (22.2%), 3 of whom were unvaccinated (Table 1). Conclusions: Superspreading infection among fully vaccinated individuals occurred in an acute-care hospital while the δ (delta) variant was dominant. Given the potential for severe complications, as this outbreak demonstrated, preventive measures including adequate ventilation should be emphasized to minimize transmission in hospitals.
Funding: None
Disclosures: None



Appropriate Number of Observations to Determine Hand Hygiene Compliance Among Healthcare Workers
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 1 / Issue S1 / July 2021
- Published online by Cambridge University Press:
- 29 July 2021, p. s64
-
- Article
-
- You have access
- Open access
- Export citation
-
Background: We sought to determine the minimum number of observations needed to determine hand hygiene (HH) compliance among healthcare workers. Methods: The study was conducted at a referral hospital. We retrospectively analyzed the result of HH monitoring from January to December 2018. HH compliance was calculated by dividing the number of observed HH actions by the total number of opportunities. Appropriate HH compliance rates were calculated based on the 6-step technique, modified from the World Health Organization (WHO) recommendation. The minimum number of required observations (n) was calculated by the following equation using overall mean value (r), absolute precision (d), and confidence interval (1-α) [The equation: n3 Zα/22×ρ×1-ρ/d2]. We considered ds of 5%, 10%, 20%, and 30%, with CIs of 99%, 95%, and 90%, respectively. Among the various cases, we focused on 10% for d and 95% for CI. Results: During the study period, 8,791 opportunities among 1,168 healthcare workers were monitored. The mean HH compliance and appropriate HH compliance rates were 80.3% and 59.7%, respectively (Table 1). The minimum number of observations required to determine HH compliance rates ranged from 2 (d, 30%; CI, 90%) to 624 (d, 5%; CI, 99%), and the minimum number of observations for optimal HH compliance ranged from 5 (d, 30%, CI, 90%) to 642 (d, 5%; CI, 99%) (Figure 1). At 10% absolute precision with 95% confidence, the minimum number of observations to determine HH and optimal HH compliance were 61 and 92, respectively. Conclusions: The minimum number of observations to determine HH compliance varies widely according to setting, but at least 5 were needed to determine optimal HH compliance.
Funding: No
Disclosures: None
Figure 1.
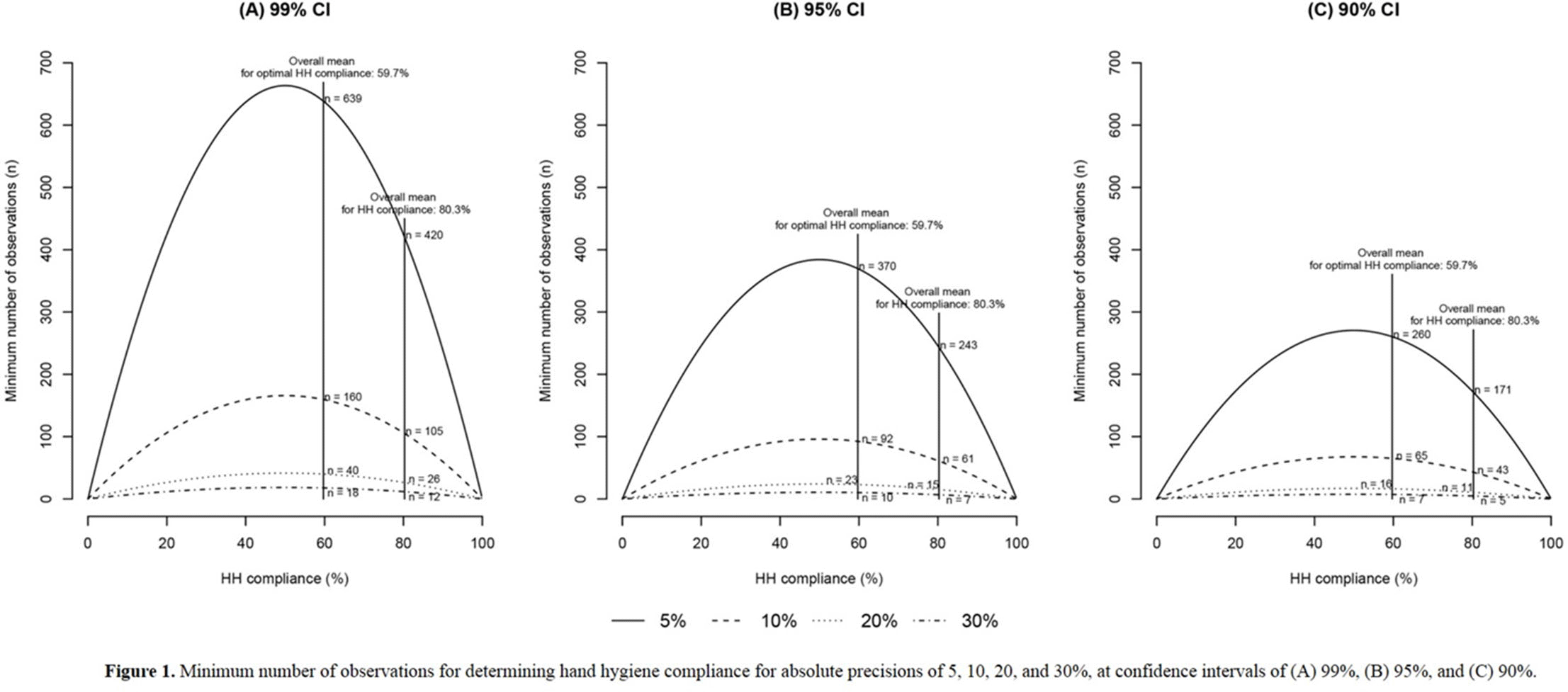
Table 1. 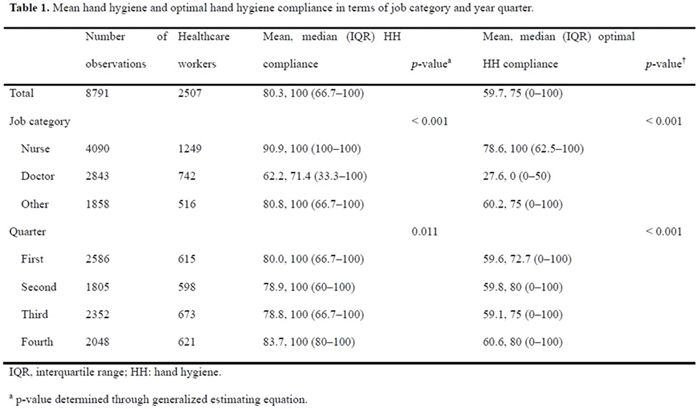


Impact of Roommates on MDRO Spread in Nursing Homes
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 41 / Issue S1 / October 2020
- Published online by Cambridge University Press:
- 02 November 2020, pp. s66-s67
- Print publication:
- October 2020
-
- Article
-
- You have access
- Export citation
Decreased Hospitalizations and Costs From Infection in Sixteen Nursing Homes in the SHIELD OC Regional Decolonization Initiative
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 41 / Issue S1 / October 2020
- Published online by Cambridge University Press:
- 02 November 2020, pp. s7-s8
- Print publication:
- October 2020
-
- Article
-
- You have access
- Export citation
EARLY ASSESSMENT AND PREDICTION OF POTENTIAL IMPACT OF THE IMPLANTATION OF POLYURETHANE SCAFFOLD IN PARTIAL MENISCAL LESIONS: A PILOT HORIZON SCANNING ACTIVITY IN SOUTH KOREA
-
- Journal:
- International Journal of Technology Assessment in Health Care / Volume 31 / Issue 6 / 2015
- Published online by Cambridge University Press:
- 18 December 2015, pp. 380-389
-
- Article
- Export citation
